
We need a referral system that works
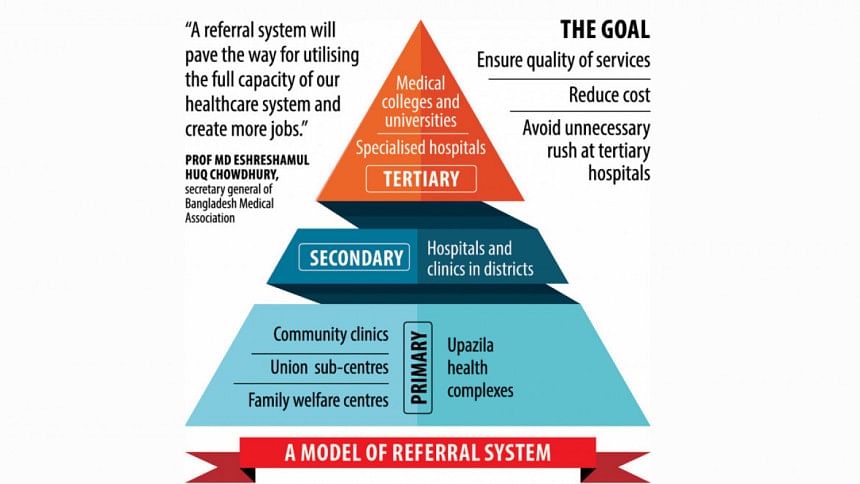
In the vibrant tapestry of Bangladesh's healthcare landscape, the urban sector faces a pressing issue: a disjointed referral system. The three-tier healthcare structure—primary, secondary, and tertiary—is grappling with a critical flaw: the urban primary healthcare services are often overlooked, prompting patients to bypass them and directly seek assistance from tertiary-level hospitals. This phenomenon places an undue burden on institutions like Dhaka Medical College Hospital (DMCH), Bangabandhu Sheikh Mujib Medical University (BSMMU) and others, resulting in a compromised service quality due to an overwhelming number of patients.
Urban areas, where the demand for healthcare is robust, find themselves hindered by a non-functional reference system. The three-tier model, designed to channel patients through primary and secondary care before reaching tertiary facilities, falters as patients opt for direct access to advanced healthcare, sidestepping primary services.
 For all latest news, follow The Daily Star's Google News channel.
For all latest news, follow The Daily Star's Google News channel. The DMCH, BSMMU, and affiliated institutes, despite their capabilities, are stretched thin due to an influx of patients seeking care for issues that could be efficiently handled at the primary level. This overcrowding poses a challenge for doctors who find themselves unable to deliver optimal services amid the patient surge.

The weakness in urban primary healthcare stems from its indirect governance structure. Unlike facilities directly managed by the health ministry, urban primary healthcare facilities operate under the jurisdiction of city corporations and municipalities, often in collaboration with NGOs through contractual agreements. This arrangement, while well-intentioned, has led to a lack of visibility and popularity for these primary care services.
To navigate this critical juncture, a strategic approach is imperative.

Acknowledging the current strain on the reference system is the first step. An in-depth analysis of patient behaviour, coupled with targeted awareness campaigns, is essential to address misconceptions and illuminate the significance of urban primary healthcare. Advocating for a shift in governance structure is also crucial. Direct oversight of urban primary healthcare by the health ministry would align these facilities with national health priorities, fostering standardisation and a more cohesive healthcare approach.
Redefining collaboration between city corporation and municipalities, NGOs, and the health ministry is paramount. Transparent governance models that facilitate effective communication and resource allocation can enhance the efficiency of urban primary healthcare.
Implementing incentives to encourage patients to adhere to the reference system is vital. Whether through reduced waiting times or other patient-friendly measures, incentivising proper utilisation of primary healthcare can alleviate the strain on tertiary hospitals.
In the challenging landscape of urban healthcare in Bangladesh, understanding the strain on the reference system is pivotal. By addressing patient behaviour, advocating for structural shifts, fostering collaboration, and incentivising proper utilisation, we can chart a course towards a more balanced and effective urban healthcare system. The focus must be on acknowledging the situation's intricacies before implementing strategic solutions for a healthier urban future.
Mahir Al Asif Masrur is a student of the Institute of Health Economics, University of Dhaka.
Views expressed in this article are the authors' own.
Follow The Daily Star Opinion on Facebook for the latest opinions, commentaries and analyses by experts and professionals. To contribute your article or letter to The Daily Star Opinion, see our guidelines for submission.









Comments