
COVID-19 and the economisation of life in Bangladesh
In today's COVID-19 stricken world, a large part of the debates on whether and how the countries should ease the lockdown is shaped by the logic of saving the economy. The Bangladesh government, for example, has started easing the lockdown restrictions to minimise the economic impact. It reminds us of a significant historical-biological-social experiment of the 20th century.
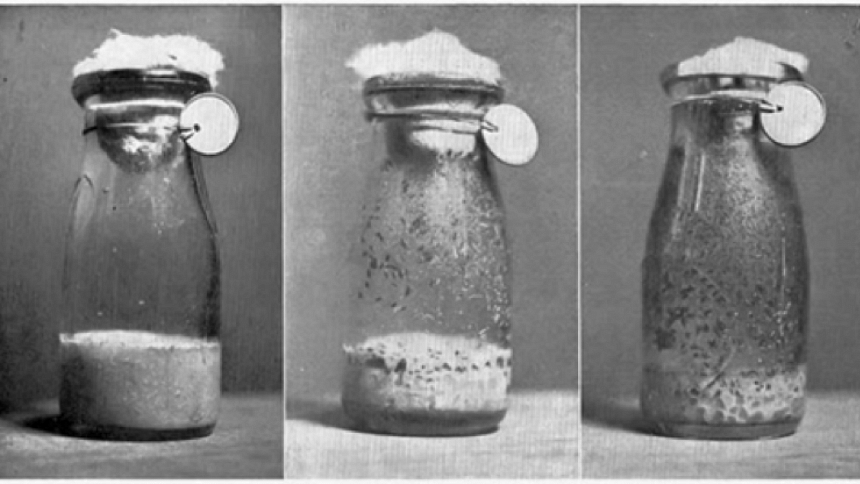
In the 1920s, American Biologist, Raymond Pearl put some Drosophila (fruit flies) in a closed bottle with some foods in his laboratory. He then plotted the number of living flies overtime on a graph and showed how their population growth saturated at one point. Soon he turned his experiment with the flies to make a universal claim on "how things grow" for all living organisms, including humans. He argued that, like the closed bottle, a national economy could only host a maximum size of the population for a more extended period. This argument was widely used by many governments as well as local and international organisations to legitimise the exploitation of racialised, female, colonised, working, and disabled bodies in the name of managing population and saving the economic futures. For example, instead of encouraging redistribution and equitable allocation of resources, many countries in the Global South were directed to "control" their population through forced sterilisations and unsafe experimental birth control methods in the 1980s and 1990s. The logic of economic development was at the heart of those top-down population control measures, which affected the bodies, health, and well-being of many women from working-class, racialised, and marginalised backgrounds.
 For all latest news, follow The Daily Star's Google News channel.
For all latest news, follow The Daily Star's Google News channel.
The economisation of life
The global COVID-19 pandemic is currently creating an abundant ground for reinforcing Raymond Pearl's logic of viewing the human population in an economic container. Countries in both the Global North and the Global South are doing a cost-benefit analysis of easing the lockdown and re-opening the economy. What is often lost in these discussions is how justifying a life by its economic worth and reducing a life into a quantifiable matrix not only strip of its beautiful familial, social, and cultural values but also make us lose our morals to the "market."
As feminist historian Michelle Murphy argues, the process of "economisation of life" ascribes values on lives that serve the purpose of the national economy. It involves a governance mechanism that selects which lives are "worth living" and "worth saving," relying on the market rationales. Hence, the lives of "less important" older adults and the "disposable" garment workers become "expendable" to feed the national dream of a burgeoning economy. Ironically though, the justification for such economisation often comes wrapped in a noble packaging of saving more lives, where the crucial question of "who will live and who will die?" remains silent.
The economised lockdown
In the wake of the coronavirus crisis, the Bangladesh government announced a "general holiday" starting from March 26, which has been extended until May 16 on several rounds. Prime Minister Sheikh Hasina issued 31 directives that laid out how lives will be governed and managed during the pandemic. For example, clause 22 specifically mentions that disadvantaged workers such as agriculture workers, day labourers, rickshaw- and van pullers, and transport workers will get special attention and relief. Nevertheless, there was absolutely no mention of nearly 4.1 million garment workers or 10.5 million domestic workers—most of whom are working-class, underprivileged women. Garment workers' labour is intrinsically hinged with the national economic interest, and domestic workers' labour is critical for sustaining middle- and upper-class lives during the pandemic, and there is an abundant supply of these cheap, feminised, disposable bodies. Therefore, the purpose of serving the economy superseded the necessity of protecting these workers from the virus. The languages of "home quarantining" and "social distancing" were directly imported from the west to save lives that were worthy of protection. Those vocabularies and concepts made little sense to those who live in slums, who work in crowded factories, who do not afford to work-from-home, who are the gendered-racialised-classed Others in our society. The calculated economised lockout reserved access to quarantining and social distancing for those who seemed worthy of living.
Life vs economy
In a society where economy becomes the container of lives, it is not surprising that the logic of national economic interests will shape the arguments around how to manage the lockdown. We are frequently seeing the simplest arguments, such as more people will die from starving or famine if the lockdown continues. To validate these claims, sophisticated economic models are often used to pinpoint the difference between the numbers of deaths if and if not the lockdown is eased.
Many have found that the binary choice between life vs economy problematic as the so-called "choice" does not question whose lives will be saved and which elements of the economy will be worth saving. The whole fear of having a famine has been questioned by many by referring to the Nobel Laureate economist Amartya Sen, who accuses the lack of democracy in a country for creating famine, and not the lack of food. Another Nobel Laureate economist, Abhijit Banerjee, stressed that countries like India should not be obsessed with macroeconomic stability during the pandemic. He proposed printing and transferring money to the people who need it the most and the adoption of a fiscally liberal economic policy. The Indian state of Kerala—which is ruled by the communist state government—has been widely praised for its efficient human-centric response to COVID-19. Along with technological measures, such as mass testing, contact tracing, and longer quarantining, Kerala distributed cooked meals to people in need, built shelters for migrant workers stranded by the unanticipated sudden shutdown, and provided broader social support to the community.
Demographic dividend?
"Demographic dividend' has often been used as a reason to open work and marketplaces in many countries. The explanation goes as follows. Since a country like Bangladesh has most of its population young, who are often believed to be less vulnerable to COVID-19 and who make the majority of the workforce, some policymakers see less risk in opening the economy and exposing the workforce to COVID-19. We argue that this argument is shallow at the best and cruel, discriminatory, and unethical at the worst. First of all, young people are also vulnerable to COVID-19, and exposing them to the virus can cause significant damage to this valuable group of our national population. In fact, 72 percent of all COVID-19 positive cases are below 50 years in Bangladesh (New Age, April 13, 2020). Second, this idea is simply cruel to older people who are still working, and this decision might be considered as workplace discrimination to them. Third, even if a young worker does not get affected by COVID-19, they can carry the virus from their workplace to their family and friends, and thus a large section of the country's population may be put in risk. Fourth, most of those economic analyses did not consider the impact of long-term disabilities and psychological trauma that COVID-19 can cause. Neither did they factor in the expenses that a family may incur if the virus hits them. Incorporating these factors may significantly change the "cost" of opening the economy before reaching an adequate level of safety. Fifth, the exposure to the virus will not be equal for workers of every social class. While some white-collar professionals can work in isolated AC rooms and use their private cars for transportation, many workers work in crowded workplaces—where social distancing protocols will be challenging to implement—and commute in crowded public transports. The latter group will suffer much more than the former, and that will be clear discrimination to the marginalised working-class people in our society.
The toll on the healthcare system
The capacity, stress, and well-being of our healthcare system have also been largely neglected in most of these market-driven analyses. Bangladesh, like many other countries in the Global South, does not have a robust healthcare infrastructure that can serve a large number of patients with COVID-19. The healthcare sector is already lacking enough PPEs, ventilators, and frontline workers. Even worse, our doctors, nurses, and other frontline medical service providers are paying a high cost while serving the patients. As of May 4, 2020, more than 554 doctors have been tested positive, and two of them died. Further losses of the lives of medical professionals will escalate the situation very quickly. Thus, a surge in the number of COVID19 patients will put the whole medical system into a severe risk of total breakdown. Also, the economic, social, and psychological losses of the healthcare workers have not been accounted for in most economic analyses that advocated for easing the lockdown. Sweden's decision to keep businesses open and rely on the strategy of developing "herd immunity" may apparently seem seductive, but Bangladesh's healthcare system is nowhere close to Sweden to tackle an overwhelming number of COVID-19 patients at a time.
COVID-19 has not only put the formal healthcare system in severe stress, but informal social support is also affected by this virus. Due to widespread panic and stigma around this virus, it is now very difficult for one to expect care from other family members, relatives, and friends if they get sick. We have already heard many anecdotes of how some COVID-19 patients could not get any support from their families, and they died alone. Without formal and informal healthcare support, thus a vast majority of people in the country may suffer from indescribable miseries from this virus if the lockdown is eased too soon. Add to that the fact that the patients suffering from other critical diseases will also be deprived of the necessary care. New York City alone recorded a death rate that is six times higher than the normal level between March 11 and April 25 (New York Times, April 27, 2020), which were directly or indirectly caused by COVID-19. In most of the cases, patients did not receive the necessary treatment as the healthcare system was overwhelmed by COVID-19. The number of excess deaths would be much higher in developing countries like Bangladesh, where the health infrastructures are much inadequate, and the population density is much higher. Where do we find these discussions in those economic analyses?
The hope
We cannot deny that saving the economy is sometimes intertwined with saving lives and livelihoods. However, drawing on Michelle Murphy's insights, we object to the tendency of perceiving the population to be trapped inside the closed bottle of the national economy and the lure of controlling and governing the size of the population to feed the market. Seeing the population through the narrow economic lens legitimises large expenditures on the production and analysis of big data, mass surveillance, deployment of privacy-breaching interventions, draconian laws to control free speech, and discriminatory policies to tackle the pandemic. A world dealing with an unprecedented crisis needs the prioritisation of the health and well-being of communities over focusing on macrological quantified measures like economic growth and productivity.
Dr Syed Ishtiaque Ahmed is assistant professor, Department of Computer Science, University of Toronto, Canada. Dr Nafisa Tanjeem is assistant professor, Global Studies and Women's, Gender, and Sexuality Studies, Lesley University, USA. Dr Ayesha Sania is associate research scientist and epidemiologist, Columbia University, USA. Dr Md Ruhul Amin is assistant professor, Department of Computer Science, Fordham University, USA.




Comments